Five strategies to improve medical training โ to reduce stress and boost expertise
April 18, 2019
Share
![[Medical students]](/gazette/sites/gazettewww/files/assets/WEB%20Luis%20Melendez-unsplash.jpg)
Recent changes in undergraduate medical education and postgraduate residency training in Canada are , increasing their debt load and reducing their experiential learning.
Such changes include a perceived shortage of residency positions, a premature requirement to choose a career path early in medical school and a growing fixation on exam preparation.
Older doctors are largely unaware of these new challenges. For trainees, on the other hand, this is the only system they know. Patients simply expect us to produce โtriple Aโ doctors โ available, affable and able.
As a cardiologist and head of medicine at Queenโs University, I offer several suggestions to reduce trainee stress, debt and burnout. I believe these suggestions will also enhance the expertise of Canadaโs newly minted doctors.
For a start, we should increase residency training positions to meet Canadaโs medical needs, and simplify the process for allocating residency positions. We should also constrain the time trainees spend studying for qualifying exams, delay the selection of medical career tracks until internship and restore the rotating internship.
Loss of empathy and self-worth
Nearly half of medical residents report burnout โ . Burnout is reported ever earlier in residents, despite legislated restrictions on work hours and increased pay.
A contributing factor is the increasing time residents spend studying for the . Trainees are also impacted by funding decisions of provincial governments, which limit the size of medical schools and residency programs, and by hospital congestion, which impairs the learning environment.
The reasons medical students experience burnout are complex. They include worries about whether they will match to a residency program and about which career track to select during their second year. Students also worry about debt โ the . This number (and many students borrow up to $200,000).
While tuition (at around $20,000 per year) is an important source of debt, a new and avoidable expense relates to the cost of off-site electives and CaRMS interviews incurred in their search for future residency positions.
1. Increase residency positions
So, what if we increased residency positions 10 per cent while reducing off-site medical school electives?
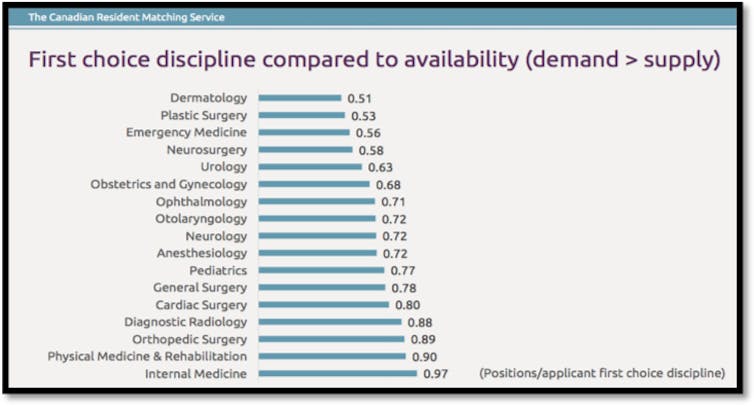
Medical students and residency training programs rank each other through an online system, called . Recently, โ from 11 in 2009 to 68 in 2017. While 68 unmatched students (from a national total of 3000) may sound like a small problem, it can have tragic consequences.
โWithout a residency position, my degree โฆ is effectively useless. My diligent studies of medical texts, careful practice of interview and examination skills with patients and my student debt in excess of $100,000 on this pursuit have all been for naught.โ
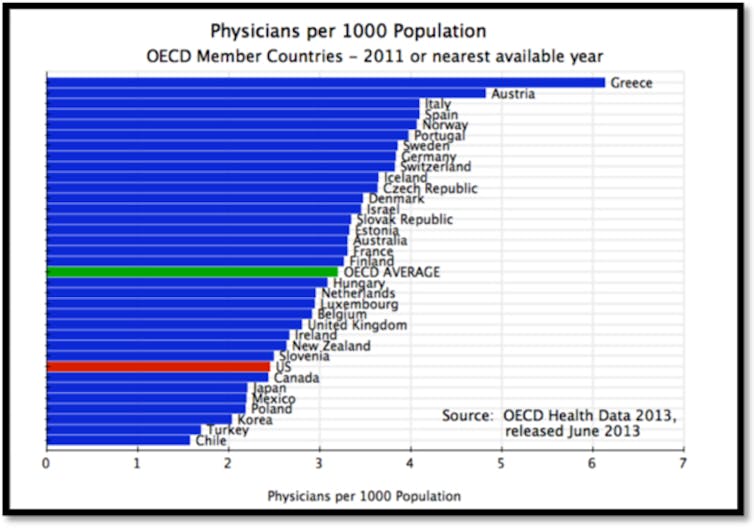
Of course, we should only create more residency positions if we need more doctors. Provincial governments tend to believe there are too many doctors; however, OECD data show Canada (with two MDs per 1,000 population) ranks near the bottom of the pack.
In 2017, there were 2,967 residency positions available in Canada and . This scarcity is exacerbated by , many of , a net and fewer available positions in โpopularโ specialty programs, such as dermatology, emergency medicine and plastic surgery.
This means that there is just two per cent wiggle room between positions required and positions available, complicated by student geographic and specialty preferences.
2. Develop a โlearn localโ strategy
To reduce the risk of being unmatched, medical students spend their time criss-crossing Canada performing electives to demonstrate their interest in a program, while serving as their own travel agent and paying for travel and accommodations.
This adds to their debt and stress and these brief sojourns often yield superficial clinical experiences. One budding dermatologist told me:
โI did six electives in dermatology (12 weeks total), and two electives in internal medicineโฆ If I was to do it again, I probably wouldnโt have done so many dermatology electives - itโs just that I didnโt get the ones I really wanted until the end. Iโm not sure I necessarily needed to do this many dermatology electives in order to matchโฆ.I definitely felt the pressure to do the majority of my electives in this specialty to show my interest and build relationships at the programs I was interested in. โฆ I canโt say exactly how much I spent. Certainly, in the thousands of dollars.โ
Another student toured 12 universities across Canada to interview for surgery residencies. She ended up with her first choice of residency and stayed at her home university. Between external electives and the CaRMS interviews, medical students lose around four months of local clinical exposure.
A โlearn localโ strategy combined with a 10 per cent increase in residency positions would reduce expense, travel and stress and allow students to extend rotations at their own centres. The proposed changes would also right-size our medical work-force.
3. Delay specialty selection
What if we delayed the choice of career track until internship?
Some students struggle to choose a speciality. Family physician, internist, surgeon, pediatrician, obstetrician, radiologist, ophthalmologist, pathologistโฆ there are many options. How can an informed choice be made after two years of relatively superficial exposure to the options?
A Queenโs student noted:
โIt felt like there was an abrupt change when we went from exploring disciplines in medical school to when we needed to decide on our specialization. In first year, we were required to do observerships to promote variety. But midway through second year we needed to select our clerkship stream and then all of a sudden it seemed like decisions had to be madeโฆ. Midway through second year, by picking my stream, I had to decide that I was not going to pursue emergency medicine, anesthesia or a subspecialty surgery.โ
By delaying specialty selection until internship, trainees could make more informed choices.
4. Reinstate the rotating internship
What if we reinstated the rotating internship?
A rotating internship gave doctors a broad experience. in favour of a two-year family medicine residency in around 1990. However, rotating internships did not just train GPs, they also trained many future specialists.
During my rotating internship at Royal Columbian Hospital in New Westminster, British Columbia, from 1981 to 1982, I spent time in obstetrics (delivering more than 100 babies), pediatrics (caring for sick and premature babies), surgery (as first assist on all operations and primary surgeon for hernias and appendectomies), intensive care (placing arterial lines and managing ventilators) and internal medicine (running the ward).
I learned respect for each specialty by walking a mile in their shoes. These practical experiences alter the medical DNA of a young physician in a way no clerkship experience can. Re-establishing a rotating internship as the first year of residency would result in Canadaโs doctors being more broadly trained.
5. Reduce preparation time for exams
Exams consume a traineeโs after-hours life for one month of medical school and nine months of residency, engendering stress and contributing to burnout. Studying too much may also distract trainees from clinical learning opportunities.
Objectively however, the for Canadian graduates (likewise the LMCC exam for medical students).
Letโs recast medical school and residency as programs for adult learners and reset expectations for how much time a trainee can or should study to some reasonable duration โ say one month for medical students and two months for residents.
The training of doctors is a joint responsibility of universities, provincial agencies, accrediting agencies and society. Together we should refocus medical school and residency training with the goal of producing triple A doctors who are more clinically experienced, less stressed and owe less money.![]()
____________________________________________________
is a professor and the head of the Department of Medicine at ฐฤรลม๙บฯฒสฟชฝฑฯึณก.
This article is republished from under a Creative Commons license. Read the .
The Conversation is seeking new academic contributors. Researchers wishing to write articles should contact Melinda Knox, Associate Director, Research Profile and Initiatives, at knoxm@queensu.ca.